Qsymia can help many adult patients you frequently see1,2
Along with diet and exercise, prescription Qsymia has been clinically proven to help a broad range of patients significantly reduce weight1,2
Along with diet and exercise, prescription Qsymia has been clinically proven to help a broad range of patients significantly reduce weight1,2

Winona,
Teacher
Actor Portrayal
Age:31
Weight:187lbs
Waist:36”
Clinical Notes
Can no longer afford GLP-1 weight management treatment after losing her commercial insurance coverage. Hopes to lose 10-15% of her weight per the treatment plan developed by her physician.
| Diet and Exercise Alone |
 Diet and Exercise with Qsymia 7.5/46 mg||
Diet and Exercise with Qsymia 7.5/46 mg|| |
 Diet and Exercise with Qsymia 15/92 mg||
Diet and Exercise with Qsymia 15/92 mg||
|
|
| (Placebo) | (Recommended dose) | (High dose) | |
| Weight Loss (% from baseline)‡ | -2 | -8 | -10 |
|---|---|---|---|
| Weight Reduction in lbs§ | -7 | -23 | -30 |
| Waist Circumference Reduction in inches§ | -2 | -4 | -5 |
| Number of Patients (N) | 383 | 233 | 424 |
†Presented here is a subset of the clinical data for patients 18 years and older (N=2,473) who participated in 1 of the 2 trials and who used study drug for the planned 56-week course of treatment. In this trial, all patients had a baseline BMI of ≥ 27 kg/m2 with additional weight-related comorbidities. See study design below. Impaired glucose tolerance/impaired fasting glucose (68% of subjects): fasting glucose > 100 mg/dL and/or > 140 mg/dL 2 hours post 75 gm glucose load in OGTT and/or diagnosis of type 2 diabetes managed with lifestyle modification or metformin therapy. ‡Source: supplementary webappendix to Gadde KM, Allison DB, Ryan DH, et al. Published online April 11, 2011.13 §Mean change from baseline. ||p<.0001 vs placebo Study Design1,2 The titration schedule for the studies was faster than what is recommended in the Qsymia package insert. Subjects took the 3.75 mg/23 mg strength for one week, then the 7.5 mg/46 mg strength for one week (unless randomized to this arm); then the 11.25 mg/69 mg strength for one week, followed by the 15 mg/92 mg strength.1,2 Data for adult patients with a BMI ≥ 27 kg/m2 after 56 weeks on recommended dose (7.5 mg/46 mg) and top dose (15 mg/92 mg) of Qsymia combined with diet and exercise. Qsymia was studied in 2 large trials supporting FDA approval that involved 3,754 adult patients whose BMI was 27 kg/m2 or greater. For the subjects in the 2 trials the average baseline weight was 256 lbs and 227 lbs, and the average baseline waist circumference was 47 inches and 45 inches. Patients were randomized to placebo, phentermine 3.75 mg/topiramate 23 mg, phentermine 7.5 mg/topiramate 46 mg, or phentermine 15 mg/topiramate 92 mg. In these trials, it was recommended that patients eat a well-balanced diet and reduce their caloric intake by 500 kcal/day. Your patients’ results may vary depending on their weight, BMI, diet, activity level, dose of Qsymia, and other factors. The titration schedule for the studies was faster than what is recommended in the Qsymia package insert. Subjects took the 3.75 mg/23 mg strength for one week, then the 7.5 mg/46 mg strength for one week (unless randomized to this arm); then the 11.25 mg/69 mg strength for one week, followed by the 15 mg/92 mg strength. See recommended dosing schedule in the Full Prescribing Information. |
After one year of treatment, patients at risk for developing diabetes had greater reductions in fasting blood glucose and insulin with both doses of Qsymia than with placebo. Qsymia is not indicated for the treatment of type 2 diabetes, hypertension or dyslipidemia.1
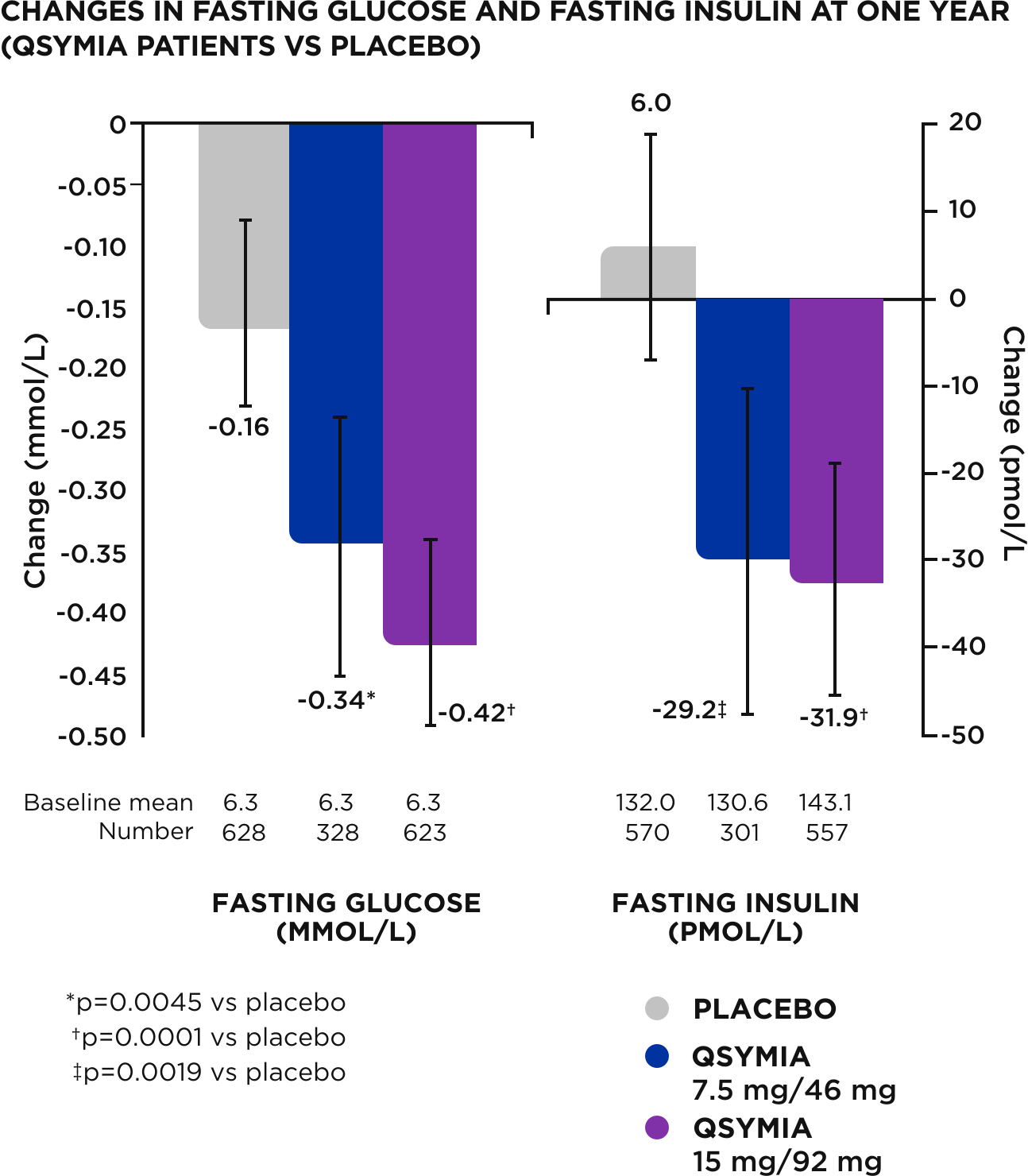
PROGRESSION TO TYPE 2 DIABETES#
The rate of progression to diabetes in patients without diabetes at baseline was also studied as part of the trial. At one year, Qsymia patients were half as likely to progress to T2D compared to placebo.
Note: Patients without diabetes were judged to have progressed to type 2 diabetes if two or more consecutive measurements showed fasting glucose concentrations of at least 6.99 mmol/L or the oral glucose tolerance test after 2 h was at least 11.1 mmol/L.
#Source: supplementary webappendix to Gadde KM, Allison DB, Ryan DH, et al. Published online April 11, 2011.13
![PRESCRIBE THE #1 NON INJECTION[SM] WEIGHT-MANAGEMENT BRAND FOR ADULTS**](/include/image/global/prescribe_non_injection.svg)



Additional resources for Healthcare Professionals
Choose once-daily Qsymia as first-line for obesity treatment — explore the following:
*Home Delivery and Retail Pharmacy
$98 home delivery pharmacy pricing includes 6-week New Patient Packs, 6-week Titration Packs and all 30-day prescriptions. Additional shipping and handling costs will apply. This is a cash only program - insurance claims will not be processed. Please see QsymiaEngage.com for full program details. LifeLine Specialty Pharmacy is NOT AVAILABLE to patients in California, Puerto Rico, Guam or the U.S. Virgin Islands. GoodRx is a wholly-owned trademark of GoodRx, Inc. and is neither sponsored by nor affiliated with the makers of Qsymia. Costco pricing and program is exclusive to Costco Members paying cash. Click here for more information on the Qsymia Retail Savings Card.
**IQVIA Reporting - Jan 2023 - Mar 2025
Indication
Qsymia is indicated in combination with a reduced-calorie diet and increased physical activity to reduce excess body weight and maintain weight reduction long term in:
Limitations of Use
Important Safety Information
Qsymia is contraindicated in pregnancy; in patients with glaucoma; in hyperthyroidism; in patients receiving treatment or within 14 days following treatment with monoamine oxidase inhibitors (MAOIs); or in patients with hypersensitivity or idiosyncrasy to sympathomimetic amines, topiramate, or any of the inactive ingredients in Qsymia.
The most commonly observed side effects in controlled clinical studies, 5% or greater and at least 1.5 times placebo, in adults include paraesthesia, dizziness, dysgeusia, insomnia, constipation, and dry mouth. Common side effects in pediatric patients aged 12 years and older at ≥4% and greater than placebo include depression, dizziness, arthralgia, pyrexia, influenza, and ligament sprain.
Qsymia can cause fetal harm. Data from a pregnancy registry and epidemiologic studies indicate that a fetus exposed to topiramate, a component of Qsymia, in the first trimester of pregnancy has an increased risk of oral clefts (cleft lip with or without cleft palate). Pregnancy testing is recommended before initiating Qsymia treatment in patients who can become pregnant and monthly during Qsymia therapy. Advise patients who can become pregnant of the potential risk to a fetus and to use effective contraception during Qsymia therapy.
Topiramate, a component of Qsymia, increases the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Patients should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior. Discontinue Qsymia in patients who experience suicidal thoughts or behaviors. Qsymia is not recommended in patients with a history of suicidal attempts or active suicidal ideation.
Acute angle closure glaucoma has been reported in patients treated with topiramate, a component of Qsymia. Symptoms include acute onset of decreased visual acuity and/or eye pain. Symptoms typically occur within 1 month of initiating treatment with topiramate but may occur at any time during therapy. The primary treatment to reverse symptoms is immediate discontinuation of Qsymia. Elevated intraocular pressure of any etiology, if left untreated, can lead to serious adverse events including permanent loss of vision.
Visual field defects (independent of elevated intraocular pressure) have been reported in clinical trials and in postmarketing experience in patients receiving topiramate. In clinical trials, most of these events were reversible after topiramate discontinuation. If visual problems occur at any time during treatment, consider discontinuing Qsymia.
Qsymia can cause mood disorders, including depression and anxiety, as well as insomnia. Patients with a history of depression may be at increased risk. For clinically significant or persistent symptoms consider dose reduction or withdrawal of Qsymia.
Qsymia can cause cognitive dysfunction (e.g., impairment of concentration/attention, difficulty with memory, and speech or language problems, particularly word-finding difficulties). Since Qsymia has the potential to impair cognitive function, patients should be cautioned about operating hazardous machinery, including automobiles.
Qsymia is associated with a reduction in height velocity (centimeters of height gained per year) in obese pediatric patients 12 to 17 years of age. Monitor height velocity in pediatric patients treated with Qsymia. Consider dosage reduction or discontinuation of Qsymia if pediatric patients are not growing or gaining height as expected.
Hyperchloremic, non-anion gap, metabolic acidosis has been reported in patients treated with Qsymia. Measurement of electrolytes including serum bicarbonate prior to starting Qsymia and during Qsymia treatment is recommended. If metabolic acidosis develops and persists, consideration should be given to reducing the dose or discontinuing Qsymia.
Qsymia can cause an increase in serum creatinine that reflects a decrease in renal function (glomerular filtration rate). In phase 3 trials, peak increases in serum creatinine were observed after 4 to 8 weeks of treatment. On average, serum creatinine gradually declined but remained elevated over baseline creatinine values. The changes in serum creatinine (and measured GFR) with short-term Qsymia treatment appear reversible with treatment discontinuation, but the effect of chronic treatment on renal function is not known. Therefore, measurement of serum creatinine prior to starting Qsymia and during Qsymia treatment is recommended. If persistent elevations in creatinine occur while taking Qsymia, reduce the dose or discontinue Qsymia.
Serious skin reactions (Stevens-Johnson Syndrome [SJS] and Toxic Epidermal Necrolysis [TEN]) have been reported in patients receiving topiramate. Qsymia should be discontinued at the first sign of a rash, unless the rash is clearly not drug related. If signs or symptoms suggest SJS/TEN, use of this drug should not be resumed, and alternative therapy should be considered. Inform patients about the signs of serious skin reactions.
The concomitant use of alcohol or central nervous system (CNS) depressant drugs (e.g., barbiturates, benzodiazepines, and sleep medications) with phentermine or topiramate may potentiate CNS depression or other centrally mediated effects of these agents. Therefore, avoid concomitant use of alcohol with Qsymia.
In situations where immediate termination of Qsymia is medically required, appropriate monitoring is recommended. Patients discontinuing Qsymia 15 mg/92 mg should be gradually tapered as recommended.
Adjust dose of Qsymia for patients with moderate or severe renal impairment. Qsymia has not been studied in patients with end-stage renal disease on dialysis. Avoid use of Qsymia in this patient population.
Adjust dose of Qsymia for patients with moderate hepatic impairment. Qsymia has not been studied in patients with severe hepatic impairment. Avoid use of Qsymia in this patient population.
Avoid the use of Qsymia with other drugs that inhibit carbonic anhydrase (e.g., zonisamide, acetazolamide or methazolamide). Use of topiramate by patients on a ketogenic diet may also result in a physiological environment that increases the likelihood of kidney stone formation. Increase fluid intake to increase urinary output which can decrease the concentration of substances involved in kidney stone formation.
Patients treated with Qsymia should be advised to monitor for decreased sweating and increased body temperature during physical activity, especially in hot weather. Caution should be used when Qsymia is prescribed with other drugs that predispose patients to heat-related disorders; these drugs include, but are not limited to, other carbonic anhydrase inhibitors and drugs with anticholinergic activity.
When prescribing Qsymia, patients should be monitored for hypokalemia. It is recommended that a blood chemistry profile is obtained at baseline and periodically during treatment.
Phentermine, a component of Qsymia, has known potential for abuse.
To report negative side effects, contact VIVUS LCC at 1-888-998-4887 or FDA at 1-800-FDA- 1088 or www.fda.gov/medwatch.
Please see the Important Safety Information, Full Prescribing Information, and Healthcare Provider Counseling Tool for Patients of Reproductive Potential for Qsymia.
Site References: 1. Qsymia Full Prescribing Information. Campbell, CA: VIVUS LLC; 2025. 2. Data on file. VIVUS LCC. 3. Contrave [package insert]. Brentwood, TN; CurraxTM Pharmaceuticals LLC; 2024. 4. Saxenda [package insert]. Plainsboro, NJ: Novo Nordisk Inc; 2023. 5. Hill AJ et al. Appetite. 1991;17(3):187-197. 6. Stubbs RJ et al. Physiol Behav. 2001;72(4):615-619. 7. Isaksson H et al. Food Nutr Res. 2008;52. 8. Pelchat ML. Appetite. 1997;28(2):103-113. 9. Hill AJ, Heaton-Brown L. J Psychosom Res.1994;38(8):801-814. 10. Garber, AJ, Abrahamson MJ, Barzilay Jl, et al. AACE comprehensive diabetes management algorithm 2013. Endocr Pract. 2013; 19(2):327-336. 11. Hampl SE, Hassink SG, Skinner AC, et al. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity. Pediatrics. 2023;151(2): 12. Bays HE, Hsia DS, Nguyen LT, Peterson CA, Varghese ST. Effects of phentermine / topiramate extended-release, phentermine, and placebo on ambulatory blood pressure monitoring in adults with overweight or obesity: A randomized, multicenter, double-blind study. Obes Pillars. 2024 Jan 8;9:100099. 13. Gadde KM, Allison DB, Ryan DH, Peterson CA, Troupin B, Schwiers ML, Day WW. Lancet. 2011 Apr 16;377(9774):1341-52.
Qsymia is indicated in combination with a reduced-calorie diet and increased physical activity to reduce excess body weight and maintain weight reduction long term in adults…
Qsymia is contraindicated in pregnancy; in patients with glaucoma; in hyperthyroidism; in patients receiving treatment or within 14 days following treatment with monoamine oxidase inhibitors (MAOIs); or in patients with hypersensitivity or idiosyncrasy to sympathomimetic amines, topiramate, or any of the inactive ingredients in Qsymia.